Why “Evidence-Based” Isn’t Just a Buzzword: A Guide to Evidence-Based PTSD Treatment
In your professional life, you demand data-driven strategies that yield measurable results. Your trauma recovery should be held to the same uncompromising standard. While the current therapeutic landscape is saturated with investigational approaches—from Brainspotting to Somatic Experiencing—that lack the rigorous backing of established science, lasting change requires empirical certainty.
Real healing depends on clinical fidelity: the expert application of gold-standard protocols like Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT). If you are seeking specialized trauma recovery care that prioritizes results over trends, the science behind your treatment is the difference between temporary relief and a permanent cognitive shift.
Before investing your time and resources into a recovery plan, it is essential to conduct the same due diligence you would apply to any high-stakes professional decision. To do that, we must first define the standard of proof.
What Does “Evidence-Based” Actually Mean?
Your time is your most valuable asset. To ensure it isn't wasted, a truly evidence-based treatment for PTSD is one that meets the following criteria:
Rigorous Testing: The treatment has been vetted through Randomized Controlled Trials (RCTs) proving the protocol itself caused the improvement, not just time or therapist attention. This means researchers randomly assigned people with PTSD to different treatments and measured their symptoms before, during, and after—using validated assessment tools, not just therapist impressions. In clinical research, RCTs are the gold standard for one reason: they provide empirical certainty. By neutralizing outside factors—luck, the passage of time, or simple supportive listening—an RCT proves that the treatment itself is the catalyst for healing.
Independent Replication: A single positive study means little. What matters is whether multiple independent research teams, at different universities and clinics across diverse, high-stress populations, keep finding the same results.
Gold-Standard Expert Endorsement: It is recommended as a first-line treatment for PTSD by organizations like the American Psychological Association (APA) and the U.S. Department of Veterans Affairs/Department of Defense (VA/DoD) which regularly review the research and publish clinical practice guidelines—essentially, their expert consensus on which treatments have earned recommendation. These aren't marketing documents; they're rigorous evaluations of the available science.
Measurable Outcomes: It demonstrates a significant, meaningful symptom change—not just that people felt good about therapy, but that PTSD symptoms measurably decreased on validated symptom measures.
Two therapies sit at the top of the evidence hierarchy as Gold Standard, First-Line Treatments for PTSD: Prolonged Exposure (PE) and Cognitive Processing Therapy (CPT). While both are trauma-focused, they leverage different mechanisms of change. Choosing between them depends on your specific symptoms and how you prefer to process information.
Gold Standard, First-Line Treatments for PTSD
Both PE and CPT are trauma-focused therapies, meaning they don't just manage symptoms; they directly address the traumatic memory and the thoughts and feelings surrounding it. This is not incidental — it's the therapeutic mechanism that drives recovery.
Prolonged Exposure (PE)was developed by Dr. Edna Foa at the University of Pennsylvania and is grounded in emotional processing theory. PE works by helping you gradually and systematically approach trauma-related memories and situations you've been avoiding. Avoidance is one of the central mechanisms that maintains PTSD — it provides short-term relief but prevents the emotional processing that leads to recovery. PE is typically delivered in 8–15 sessions with a trained therapist. For the person who wants to face the problem head-on, PE is efficient, intensive, and arguably the most powerful tool we have for rapid symptom reduction and lasting change.
Cognitive Processing Therapy (CPT) was developed by Dr. Patricia Resick and addresses the way traumatic experiences can alter our core beliefs — about safety, trust, power, esteem, and intimacy. Many trauma survivors develop thoughts like "It was my fault," "The world is completely dangerous," or "I am permanently damaged." CPT helps you identify these "stuck points" and examine them carefully. Like PE, it is delivered in approximately 12 structured sessions.
Both PE and CPT require courage and active participation. They are not comfortable therapies. They ask you to engage with painful material rather than avoid it. But that discomfort is purposeful—it's the pathway through, not around, the trauma, ensuring that when therapy ends, the results remain. For further discussion on this, see my blog post on Why Trauma Therapy Is Hard—And Why Its Worth It.
Which Approach is Right for You?
While both PE and CPT are considered first-line treatments for PTSD, choosing between them depends on your specific symptoms and how you prefer to process information.
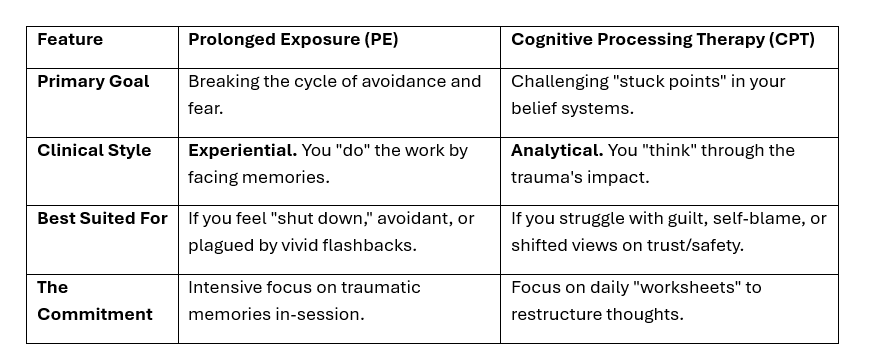
A Comparative Analysis of PE vs CPT
To help you weigh your options with even greater precision, the Department of Veterans Affairs National Center for PTSD offers an interactive PTSD Treatment Decision Aid. This tool allows you to compare the best available treatments side-by-side, watch videos of experts explaining the protocols, and build a personalized summary to bring to our initial consultation. It is an excellent resource for those who want to ensure their recovery plan is backed by the highest level of clinical evidence.
Evaluating Other Approaches: Where Does the Science Stand?
When you search for PTSD therapists online, you'll encounter many other approaches. Many of therapies are marketed as "gentler" alternatives, but they often lack the empirical backing required for a reliable recovery. Many therapists in the community offer "trauma-informed" care, but "informed" is not the same as "evidence-based." Here is a breakdown of common approaches and where they stand in the evidence hierarchy.
Second-Line Treatments for PTSD
Eye Movement Desensitization Reprocessing (EMDR): EMDR processes memories using bilateral stimulation (such as guided eye movements, sounds, or taps) while you are in a safe, controlled environment, reducing the emotional charge. According to expert consensus practice guidelines, EMDR is considered a second-line treatment for PTSD. It may be a reasonable choice. However, like PE and CPT, it requires specific training and is most effective when delivered with fidelity.
Popular but Unproven (Not Recommended)
Brainspotting: Brainspotting is an alternative therapeutic method that identifies specific eye positions—or "brainspots"—believed to correlate with unprocessed trauma in the subcortical brain. While it has gained popularity for its focus on “physiological release,” it currently lacks the robust, peer-reviewed research base required for recommendation by any major clinical practice guidelines for PTSD. Existing studies are small, often conducted by brainspotting's own proponents, and frequently published outside of peer-reviewed mainstream journals. Many people receiving brainspotting may improve due to the natural effects of therapeutic attention, time, and the common elements it shares with better-studied approaches.
Tapping: Thought Field Therapy (TFT) and Emotional Freedom Techniques (EFT) involve tapping specific sequences on acupuncture meridian points to eliminate "perturbations" in the body’s energy field—a concept proponents claim is the root cause of emotional distress. While TFT uses complex, individualized "algorithms" and EFT utilizes a simplified, universal tapping circuit, both lack the empirical validation required for recommendation by any major clinical practice guidelines for PTSD. Despite being marketed for rapid relief, current science suggests that if these "energy psychology" methods show any benefit, it is likely due to the common elements they share with established treatments—such as systematic desensitization and exposure—rather than the tapping protocols themselves. Neither the APA nor the VA/DoD guidelines recommend TFT or EFT as a treatment for PTSD.
Somatic Experiencing (SE), Sensorimotor Psychotherapy (SP), and Polyvagal-Informed Therapies: These approaches focus on the "bottom-up" processing of trauma by prioritizing physiological sensations and nervous system regulation over cognitive insight. Somatic Experiencing emphasizes discharging "trapped" survival energy, while Sensorimotor Psychotherapy addresses trauma-related postural habits and physical defense responses. Polyvagal-informed techniques specifically target the vagus nerve to shift the body out of chronic "fight-flight-freeze" states.
While these methods provide valuable tools for improving mind-body connection, they currently sit in the Supplemental or Investigational tier of the evidence hierarchy. They lack the large-scale, independent RCTs necessary to prove they can consistently drive full PTSD remission on their own. As of 2026, no major clinical guidelines recommend them as standalone or first-line treatments. They may be best utilized as adjuncts to support regulation while engaging in gold-standard, trauma-focused work.
Why “Fidelity” and Specialization Matter
If you were undergoing a specialized medical procedure, you would want the surgeon who follows the proven protocol to the letter. PTSD recovery is no different.
Even when a therapist offers PE or CPT, there's an important nuance: how well they deliver it matters enormously. Both treatments are structured, manualized protocols developed through decades of research. They were designed with specific components, sequencing, and pacing that are part of what makes them work. A therapist who attended a weekend workshop in PE or CPT and then blends it loosely with other approaches is not delivering the treatment that was proven to work in trials.
A Word on Comfort and Difficulty
One reason fringe therapies sometimes feel more appealing is that they tend to be marketed as gentler alternatives to the discomfort of trauma-focused therapy. It's true that PE and CPT require you to engage with difficult material—and that this is challenging. But the research is equally clear: treatments that work for PTSD are those that help you process the trauma, not those that help you feel comfortable while the trauma remains unprocessed.
This doesn't mean your comfort doesn't matter. A good PE or CPT therapist will prepare you thoroughly, work at a pace appropriate for you, and support you through the difficult moments. The goal isn't suffering — it's liberation from PTSD, and the path there runs through the trauma, not around it.
What to Look For in a PTSD Specialist
Specific training in PE and/or CPT — not just familiarity, but formal training from an accredited program
Have you completed a formal training program for PE or CPT, including consultation with a certified trainer?
A track record of using these treatments with people who share your type of trauma
How many clients have you treated with this protocol?
Transparency about their approach — a good therapist will explain what they're doing and why
Do you follow the manualized protocol for PE or CPT, or do you use an 'eclectic' approach?"
Outcome monitoring — many evidence-based practitioners track symptom scores over the course of treatment
How do you track and measure my progress - do you use validated symptom scales?
You deserve a therapist who can tell you not just what they offer, but why the evidence supports it — and who can answer honest questions about the limitations too.
In Summary
PTSD is a serious but treatable condition. The treatments with the strongest evidence—Prolonged Exposure and Cognitive Processing Therapy—have been tested across hundreds of clinical trials, across decades, across diverse populations, and are endorsed by every major clinical guideline body. That evidence was hard-won and means something real.
Brainspotting, tapping, and somatic/polyvagal therapies may be heavily marketed, and many of their practitioners are caring people. But "caring " and "evidence-based" are not synonyms. When it comes to your mental health, you deserve both.
Finding a Specialist in Prolonged Exposure
If you are looking for a therapist who offers Prolonged Exposure (PE), it is essential to choose a provider with formal, accredited training and a commitment to clinical fidelity. At Polusny Therapy, we specialize in delivering this gold-standard protocol with the precision required to drive measurable recovery. Based in Minneapolis, we provide expert trauma care virtually across 43 PSYPACT states, ensuring that high-stakes professionals can access elite, evidence-based treatment regardless of their location.
Not sure which approach fits your needs? Take the VA Decision Aid and bring your results to our first session.
About the Author
Melissa Polusny, PhD, ABPP, is a board-certified clinical psychologist specializing in trauma and PTSD. She received extensive training in PE from its developers at the Center for Treatment and Study of Anxiety at the University of Pennsylvania. She has been a certified PE therapist, trainer, and consultant for two decades and trained hundreds of mental health professionals within the Department of Veterans Affairs. As a scientist-practitioner, she has published over 150 peer-reviewed articles related to trauma, PTSD, and resilience. Dr. Polusny is the founder of Polusny Therapy and offers private-pay, high-quality evidence-based trauma recovery in Minneapolis and across 43 states via PSYPACT.